The recent remission of HIV in a Toronto patient following a bone marrow transplant for leukemia is not a medical miracle, but a specific outcome of high-risk cellular engineering. This case represents a rare convergence of oncological necessity and virological opportunity. To understand why this remains an outlier rather than a standard of care, we must examine the biological barriers, the donor-recipient compatibility matrices, and the brutal trade-offs of the graft-versus-host response.
The Genetic Selection Filter: The CCR5-Δ32 Mutation
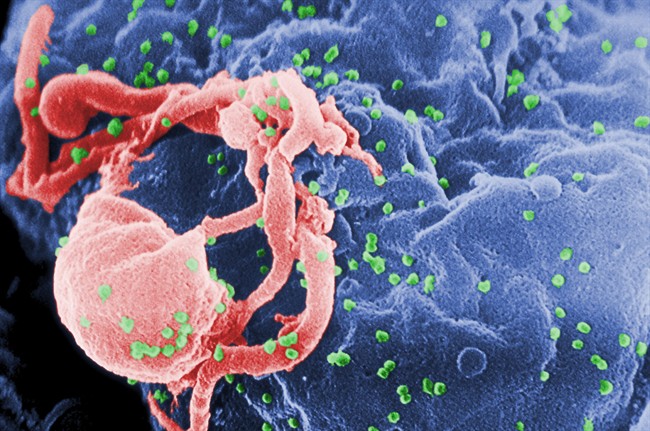
The foundational mechanism of this remission rests on the CCR5-Δ32 mutation. HIV typically enters CD4+ T cells by binding to the CCR5 co-receptor. A specific 32-base-pair deletion in the CCR5 gene results in a truncated protein that never reaches the cell surface, effectively locking the door against the virus. If you enjoyed this article, you should check out: this related article.
This mutation is rare. Roughly 1% of people of Northern European descent carry two copies (homozygous) of this mutation. Finding a donor who is both an HLA (human leukocyte antigen) match for the patient’s cancer treatment and a homozygous carrier of CCR5-Δ32 creates a statistical bottleneck. The probability of finding this "double-match" is often less than one in a million for non-European populations, highlighting a systemic inequity in the current therapeutic landscape.
The Three Stages of Viral Clearance
The remission process functions through three distinct, overlapping phases of biological attrition. For another perspective on this event, see the latest coverage from Psychology Today.
- Cytoreductive Conditioning: Before the transplant, the patient undergoes high-dose chemotherapy or radiation. While the primary goal is to ablate the patient's cancerous bone marrow, this process simultaneously destroys a significant portion of the reservoir of HIV-infected T cells. It is a scorched-earth policy that reduces the viral load to near-undetectable levels before the new immune system is introduced.
- The Genetic Barrier: The introduction of CCR5-Δ32 stem cells ensures that any new T cells produced by the graft are inherently resistant to R5-tropic HIV strains. This prevents the virus from "seeding" the new immune system.
- Graft-versus-HIV-Reservoir (GvHR): This is the most critical and dangerous phase. As the donor's immune system (the graft) engrafts, it recognizes the recipient's remaining cells as foreign. This includes the "latent reservoir"—resting cells that harbor the HIV genome but are not actively producing virus. The donor cells attack and eliminate these residual pockets of infection.
The CXCR4 Escape Tactic
A significant risk factor in these procedures is viral tropism. While most HIV strains use the CCR5 receptor (R5-tropic), some can evolve to use the CXCR4 receptor (X4-tropic). If a patient harbors even a minute population of X4-tropic virus, the CCR5-Δ32 transplant will fail to provide a cure. The virus simply switches its entry point, bypassing the genetic shield. Rigorous pre-transplant deep sequencing of the viral population is mandatory to assess this risk, yet current assays cannot always detect ultra-low-frequency X4 variants hidden in deep tissue reservoirs.
The Morbidity-Mortality Trade-off
Bone marrow transplantation is not a viable "cure" for the general population of 39 million people living with HIV because the procedure carries a treatment-related mortality rate of 10% to 20%. In a clinical environment where Antiretroviral Therapy (ART) allows for a near-normal life expectancy with a single daily pill, the risk-adjusted return on a transplant is negative for anyone not facing a terminal malignancy.
The "Toronto Patient" and previous cases like the "Berlin" and "London" patients were all treated for life-threatening blood cancers. The transplant was an oncological necessity; the HIV remission was a secondary, high-stakes objective.
Quantifying the Latent Reservoir
The primary obstacle to a scalable cure is the latent reservoir. HIV integrates its DNA into the host genome. Even when blood tests show "undetectable" viral loads, the virus persists in:
- Lymph nodes
- The central nervous system
- The gastrointestinal tract
- Resting memory CD4+ T cells
The Toronto case demonstrates that total replacement of the hematopoietic system can deplete this reservoir, but it does not clarify if the virus is truly eradicated or merely suppressed below the limit of detection for years. The distinction between "remission" and "cure" is a function of time and the sensitivity of our diagnostic tools.
Scaling the Strategy: From Transplantation to Gene Editing
Since the donor-matching process is a logistical failure for global scaling, the strategy must shift from finding resistant cells to creating them. There are two primary avenues currently under investigation that utilize the logic of the Toronto case without the lethal risks of a full transplant.
- Ex Vivo Gene Editing: A patient’s own stem cells are harvested, and CRISPR-Cas9 or Zinc Finger Nucleases (ZFNs) are used to knock out the CCR5 gene. These modified, resistant cells are then infused back into the patient. This eliminates the risk of Graft-versus-Host Disease (GvHD).
- In Vivo Gene Delivery: Utilizing viral vectors or lipid nanoparticles to deliver gene-editing machinery directly into the body to modify T cells and their precursors in situ. This bypasses the need for any hospital-intensive transplant infrastructure.
The Bottleneck of Allogeneic Immunity
While the Toronto patient is currently in remission, the durability of this state depends on "chimerism"—the degree to which the donor's cells have replaced the host's. If the host's original, susceptible cells begin to repopulate, the viral reservoir can rapidly re-establish itself.
Furthermore, the immunological "honeymoon period" post-transplant is often maintained by immunosuppressive drugs to prevent GvHD. These drugs themselves may play a role in modulating viral replication, though the exact correlation remains under investigation.
The strategic priority for the next decade of HIV research is the transition from "replacement" to "modification." The Toronto case proves that the CCR5-Δ32 mechanism is a valid target for functional cure, but the delivery mechanism (allogeneic transplant) is an obsolete vehicle for widespread application. Efforts must be concentrated on refining the precision of CRISPR-mediated CCR5 ablation to achieve similar "shielding" effects with the safety profile of a standard outpatient infusion.
Investing in HLA-diverse biobanks or universal "off-the-shelf" CAR-T cell therapies modified with CCR5 deletions represents the most logical path toward democratizing the results seen in these rare transplant cases. The medical community should treat these transplant remissions not as repeatable procedures, but as proof-of-concept benchmarks for the efficacy of genetic resistance.



